Visualizing the Inside Journey of Recovery from Opioid Use Disorder
Code for Philly 2020 Opioid Data Hackathon project to better understand recovery from opioid use disorder.

Referral process pipeline (PDF)
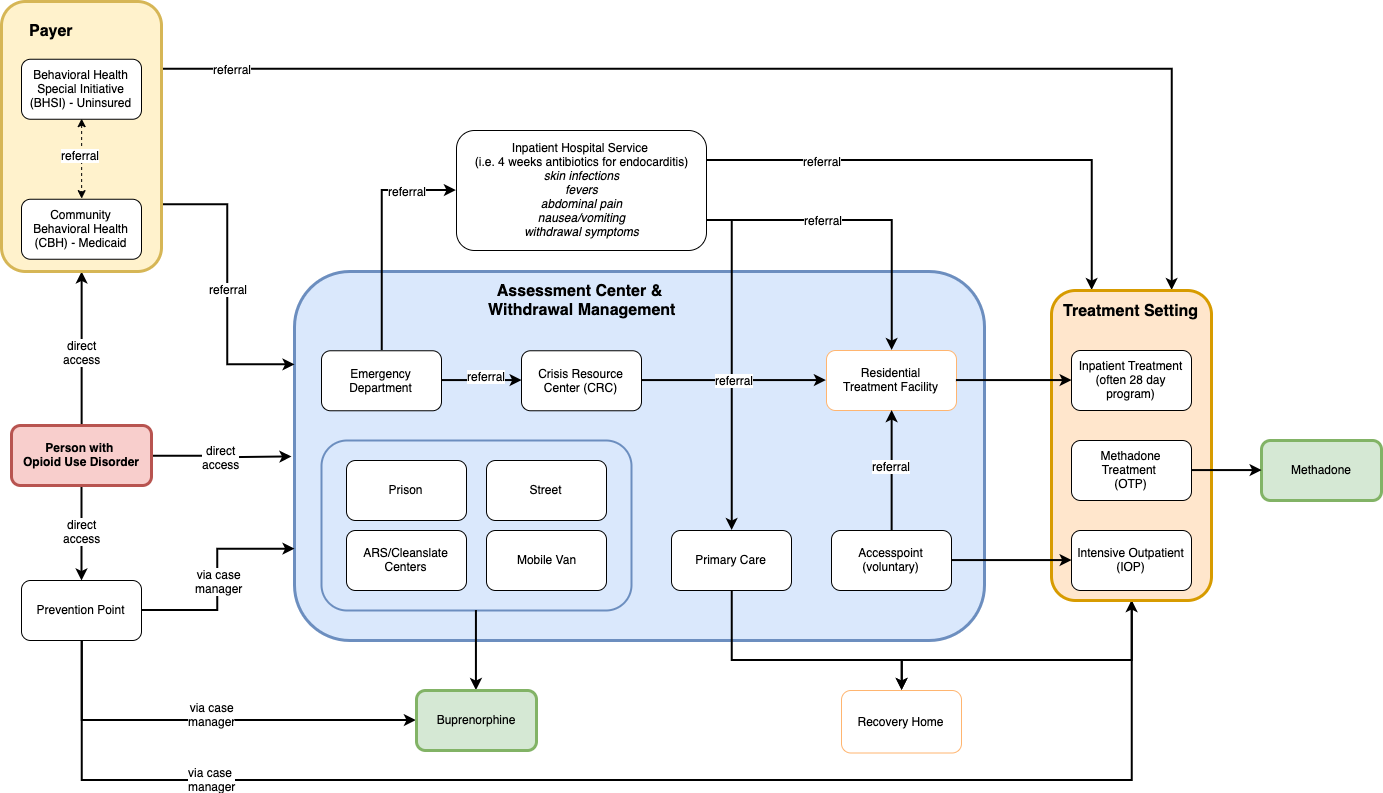
Figure 1: Schematic representation of the Medication Assisted Treatment (MAT) referral process pipeline as part of the recovery for someone with Opioid Use Disorder (OUD)
2020 Opioid Data Hackathon
This year I participated in the 2020 Opioid Data Hackathon as part of a team tasked with creating ways to visualize the opioid use disorder recovery process to identify barriers and build understanding in the general public.
I went into it thinking I might explore some interesting datasets to generate maps, and my teammates were on a similar wavelength. It didn’t take long to realize the kind of information needed to understand what it’s like to engage in recovery didn’t live in quantitative datasets. So we endeavored to collect our own qualitative data instead! We conducted interviews with our partner organizations and other major players in Philly as part of this storytelling project.
Our team’s final report, presentation, and “scrollytelling” mock-up are linked above. A slide deck created for a lab meeting presentation is also linked, and summarizes the content.
Be sure to check out these Freakonomics Radio podcast episodes to learn more about the opioid crisis in Philly:
Data Hack hosts
Partner organizations/interviewees
- Prevention Point Prevention: drop-in, medical, mobile clinic, and re-entry case managers.
- Health Federation of Philadelphia: Opioid Response Program Coordinator and intern.
- Penn Medicine Center for Opioid Recovery and Engagement: Certified recovery specialists, emergency medicine physician, and individual in recovery.
Overview
Recovery from opioid dependency often is a long and difficult journey, and it will look different for different people. For some, recovery can mean reducing dependency to a minimal level that allows them to successfully maintain their emotional, social, and economic daily life. While many programs are in place to help, recovery is a voluntary commitment from a person who might need continual encouragement and understanding, as well as assistance navigating hurdles they might not be able to overcome on their own, especially if they are going through the agony of withdrawal. Managing withdrawal symptoms is a first step toward long-term treatment, and not recognizing this need and responding to it with compassion and respect can waste an opportunity that might not come around again. Likewise, a failure to provide understanding or timely referrals at any critical point along the recovery process can lead to relapses, creating a vicious cycle of continuous addiction. Understanding what people are going through and what they need are the keys to helping people on their journey toward sustained recovery.
Recurring Themes in Recovery
We observed a number of recurring themes in the qualitative data collected.
- Every recovery path is unique. Often, a person’s recovery is non-linear, includes setbacks and does not have a clear end point. This can make visualizing a journey difficult, because there is no “typical” recovery.
- The perfect recovery process is the one perfect for that person. The best recovery process is one that meets an individual exactly where they are, free of external barriers and judgment, and full of respect and compassion.
- Relapse can happen during recovery. An individual can relapse but this does not mean that their recovery is over.
- Mindset for recovery. Recovery can only begin when a person is ready. Until that point, their access to harm reduction education and harm reduction services is extremely important.
- Role of long-term relationships between individuals with OUD and agencies that provide recovery services. Thanks to these long term relationships, a person knows where to turn when they are ready for help.
- Stigma and recovery. If an individual was treated poorly in the past by an emergency response person or at a healthy clinic, they may refuse treatment in the future. Some abstinence-based treatment programs do not condone substance use of any kind, including MAT. Stigma exists within advocacy in the form of promoting Vivitrol, which has disadvantages when compared to buprenorphine, but cannot be diverted.
- Benefit of “Lived Experience”. When case managers can share that they have “lived experience” and are in recovery themselves, it often makes individuals more comfortable. These case managers are able to offer compassion because they have been through withdrawal and some of the same challenges themselves.
- Vulnerable Populations. While there may not be a typical recovery story, it is certain that there are populations for whom there exist even more obstacles to recovery. These vulnerable populations include: homeless, uninsured, mothers, formerly incarcerated, and people with a dual diagnosis of OUD and mental illness.
Marie Ouellet
Assistant Professor
Dr. Marie Ouellet’s research focuses on delinquent groups, including how they emerge and evolve, and how networks structure this process. She is currently leading a longitudinal study on police networks to better understand the informal structure of policing, including organizational cohesion and fragmentation within departments, and the consequences of these network structures on the diffusion of behaviors and attitudes. Ouellet’s work has been published in Criminology, Criminology & Public Policy, Journal of Research in Crime and Delinquency, and Justice Quarterly.